The Centers for Disease Control has found children with disabilities have a 38% higher risk of obesity than children without disabilities (Office of Special Education and Rehabilitative Services, 2011).
Why is physical activity important?
Physical activity is a vital and necessary part of life for people of all ages. It is especially important for children with disabilities. Studies have shown participation in physical activity improves physical and mental health, along with promoting inclusion with peers.
Improvements in Overall Physical Health
Weight Loss
Increased Strength and Cardiovascular Endurance
Improved Flexibility, Balance and Agility
Reduced Risk of Developing Further Medical Conditions
Inclusion with Peers
Improved Social Skills
New Friendships
Teaches Competitiveness and Teamwork Skills
Mental Health Benefits
Increased Self-Confidence
Promotes Independence
Reduced Symptoms of Anxiety and Depression
Achievement of Goals
Physical activity provides many benefits for children with disabilities. The U.S. Department of Health and Human Services recommendation for physical activity is at least 60 minutes daily of moderate to vigorous intensity for all children (Office of Special Education and Rehabilitative Services, 2011). The significant physical and psychosocial benefits activity can have on a child with disabilities can range from improved motor coordination and weight loss to increased self-esteem and decreased risk of depression. Participation in physical activity has also been shown to have an influence on a child’s social skills. These benefits all have the possibility to have a drastic impact on the life of a child with disabilities.
Murphy, N. A., Carbone, P. S., & Council on Children with Disabilities. (2008). Promoting the participation of children with disabilities in sports, recreation, and physical activities. American Academy of Pediatrics,121(5). doi:10.1542/peds.2008-0566
Many people have talked about free play having a positive affect on children’s development, but is this a fact? Lets take a look at what the media has to say, and then examine the evidence.
But first…what is free play?
Free play can be defined as unstructured, voluntary, child-led activity that allows children to develop their imaginations while exploring and experiencing the world around them. It is the spontaneous play that comes naturally from children’s curiosity, love of discovery, and enthusiasm.
Times are changing, and the amount of free play children are engaging in is decreasing. Kids are spending less time outdoors as technology continues to take over. Many children are spending most of their time on Ipads, cell phones and video games inside of their homes. Not only are children engaging in less free play at home, but also in school environments. Numerous studies describe the disappearance of recess (unstructured, outdoor-based play during the school day) in American schools (Mainella, Agate & Clark, 2011).
Should kids be spending more time outside engaging in free play, and does this affect their development? It is a question that many parents, caregivers and educators would like to know!
The Media
The Mayo Clinic News Network reported on the importance of free play on children’s development in 2018. They discuss findings from a recent report from the American Academy of Pediatrics.
CBC News reports on a Manitoba daycare in 2017 that has its kids spend most of their time outdoors, based on the “Forest and Nature” program. Benefits such as imaginative play and social skills are discussed.
In 2016, Jennifer Hsu reports from WNYC on two kindergarten teachers that are expanding “unstructured outdoor-play” for the children at a public school in Brooklyn, NY.
What does the research say?
Does free play affect children’s development? Research suggests,
YES.
Warner (2008) speaks of the current research of play and how it is a crucial part of the development of young children. A 2006 report from the American Academy of Pediatrics said free and unstructured play is healthy and, in fact, essential for helping children reach important social,emotional, and cognitive developmental milestones as well as helping them manage stress and become resilient.
Mainella, Agate and Clark (2011) outlined the positive effects of outdoor free play on child development in the areas of physical fitness, mental health, socioemotional and cognitive development.
Kernan & Devine (2010) spoke on the importance of outdoor free play in supporting children’s well-being, learning and development, and Warner (2008) explains that children can learn to reconcile their inner world with outer reality, work to attain mastery over their environment, and learn social rules or norms from play
The takeaway…
It is a big fact that children are engaging in less free play, especially outdoor free play. With so many barriers to free play such as technology and academic standards, children are spending most of their time indoors, either at home or inside of a classroom. How can we promote healthy development for children?
We can spread our knowledge about the benefit of free play on social, emotional, cognitive and physical development and advocate for more free play and outdoor free play just as the media clips demonstrated above.
it’s time to get unstructured!
References
Kernan, M., & Devine, D. (2010). Being Confined within? Constructions of the Good Childhood and Outdoor Play in Early Childhood Education and Care Settings in Ireland. Children & Society, 24(5), 371–385. https://doi.org/10.1111/j.1099-0860.2009.00249.x
As of October 1'st 2019, PDPM( Patient-Driven Payment Model) came into place in the nursing home setting. PDPM is how a facility is reimbursed for services from insurance. Before PDPM therapy was its own entity and a facility was provided a rate depending on the coverage and amount of minutes a patient tolerated provided by therapy. This new payment model groups nursing and therapy as one.
The issue with this new system is that patients are no longer receiving therapy services like Occupational, Physical, or Speech services they require. The frequency of five times a week has been reduced to three times a week, sixty minute treatments have been cut to thirty-minute treatments, and individualized therapy is now a required group session. Instead of receiving therapy services, a skilled intervention, many facilities are implementing a restorative program six times a week into there daily documentation. By doing this, it will increase the capitalization of funds provided by PDPM. As long as a facility is providing two restorative programs a day for fifteen minutes, six days a week per CMS( The Centers for Medicare & Medicaid Services) regulations, the facility will qualify for more financial reimbursement.
A restorative program was intended initially to provide a non-skill service; it's a maintenance program to prevent falls, declines, donning splints to prevent contractures. These programs are delivered when a patient is off of therapy services; it is implemented by a therapist. With the new payment model, this is now performed in tandem. Many facilities are incorporating the restorative program in with the documentation and daily care already provided, stating the services like ADL's ( activities of daily living such as dressing, brushing teeth and eating,) and ambulating( walking) to the bathroom are enough. These are everyday skills, and no other program is put in place. What benefit is the patient getting from this?
The video intended to educate staff and patients on PDPM, about the restorative program displayed many therapeutic interventions. What is your take on the new PDPM restorative program? Do you see a bennifit? Did you know about the new restorative program in your facility? Are they billing for one?
References
Bonanni, D. R., Devers, G., Dezzi, K., Duerr, C., Durkin, M., Hernan, J., & Joyce, C. (2009). A dedicated approach to restorative nursing. Journal Of Gerontological Nursing, 35(1), 37–44. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=19227101&site=ehost-live
Remsburg, R. E., Armacost, K. A., Radu, C., & Bennett, R. G. (2001). Impact of a Restorative Care Program in the Nursing Home. Educational Gerontology, 27(3/4), 261–280. https://doi.org/10.1080/036012701750194987
vAPING IS THE NEW FAD FOR TEENAGERS AND YOUNG ADULTS
Vaping is know as an alternative to cigarette smoking. In 2014 vaping companies such as “Juul” started displaying advertisements about vaping to their targeted audience, teenagers. The advertisements in magazines and TV commercials state that vaping is a healthier alternative to smoking cigarettes. A vape cigarette pen is a device that resembles that looks like an usb that you would plug into your computer. The vape pen vaperizes oils that contain nicotine without the tobacco and other chemicals that are terrible for your lungs.
Advertisements in 2014 make the vape pens look like a healthy, fun and hip alternative to cigarette smoking.
The video above is an advertisement that is displaying a positive effect on vaping. This video displays views of capers looking as:
healthy individuals
vaping as a recreational activity without consequences
a tool to help an individual quick smoking
young adults looking “cool” as they smoke the vape pen
In 2018 there have recently been new views on vaping and the negative effects it has had on society, teenagers and young adults.
In 2018:
1 in 5 high school students are using vaping pens
1 in 20 middle schools are using vaping pens
3.6 million students are engaging in the use of vaping pens…
Evidence based articles recently state the negative effects that vaping pens have on individuals and the long term effects that are not stated in advertisements towards young teens.
Vaping is now classified as a “gate way” drug to smoking cigarettes, individuals who start vaping are more likely to start smoking cigarettes
Although vaping pens do not contain tobacco, they contain chemicals and other unhealthy oils
Vaping has long term health complications including: shortness of breath, inflamed lungs, lung disease and respiratory problems
The media may be displaying a positive image on vaping, but evidence based research has proved that vaping is not as healthy for you as perceived!
References:
Sherratt, F. C., Newson, L., & Field, J. K. (2016). Electronic cigarettes: a survey of perceived patient use and attitudes among members of the British thoracic oncology group. Respiratory Research, 17(1), 55. https://doi.org/10.1186/s12931-016-0367-y
Van Gucht, D., & Baeyens, F. (2016). Health professionals in Flanders perceive the potential health risksof vaping as lower than those of smoking but do not recommend using e-cigarettes to their smoking patients. Harm Reduction Journal, 13(1), 22. https://doi.org/10.1186/s12954-016-0111-4
Wang, J. B., Olgin, J. E., Nah, G., Vittinghoff, E., Cataldo, J. K., Pletcher, M. J., & Marcus, G. M. (2018). Cigarette and e-cigarette dual use and risk of cardiopulmonary symptoms in the Health eHeart Study. Plos One, 13(7), e0198681. https://doi.org/10.1371/journal.pone.0198681
The thought of going under the knife is frightening to most people which usually leads to patient’s avoiding surgery and dealing with their circumstances. This is very common in people who are suffering with excruciating hip pain. According to the Agency for Healthcare Research and Quality, more than 300,000 hip replacements are done each year in the United States and only a small 1% of them fail and require a revision. Usually the patient’s who require a revision are ones who are noncompliant with their hip precautions, lack the knowledge of what tools to use during healing, or may have gotten an infection. Following your precautions and having access to adaptive equipment are simple ways to avoid further injury and promote healthy healing.
What Can Lead to a Hip Replacement?
A hip replacement may be needed after having a traumatic injury (i.e. car accident or a bad fall) however, the main culprit is usually arthritis.
Arthritis itself means inflammation in a joint and there are several different kinds of arthritis. The different types of arthritis that may lead to the need for joint replacement include:
Osteoporosis- is an ailment in which bones become very weak and break easily.
Rheumatoid Arthritis- is a chronic inflammatory disorder which effects many joints including ones in hands and feet.
Osteoarthritis- occurs when the stretchy tissues around the bones are worn down.
How Would You Know if You Need a Hip Replacement?
Usually your orthopedic doctor and/or surgeon would be the one to decipher whether or not a hip replacement is necessary or if another intervention would be more appropriate. Some signs that may indicate that it is time for a hip replacement include:
Hip pain while at rest, during, or after exercise
Stiffness in your hip
Pain medication aren’t providing you the relief you want
Hip pain prevents you from doing your everyday tasks
Hip pain keeps you from engaging in your leisure activities
You’re not as mobile as usual
You have been diagnosed with arthritis in your hip
X-Rays show damage to joint
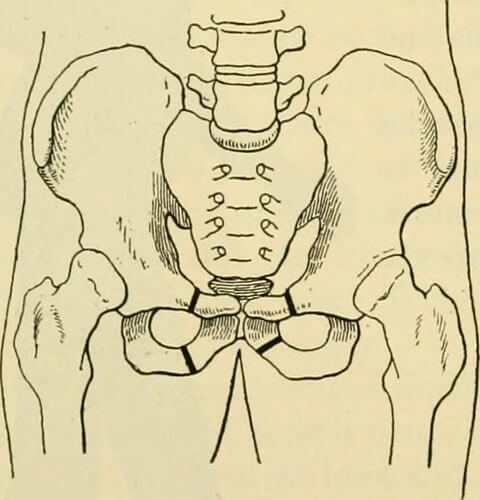
What are the Hip Precautions?
Depending on what type of hip replacement your surgeon performs, posterior or anterior (other approaches may be used), you may a different set of rules to abide by.
Anterior Hip Precautions May Include:
Do not step backwards with surgical leg. No hip extension.
Do not allow surgical leg to externally rotate (turn outwards).
Do not cross your legs. Use a pillow between legs when rolling.
Sleep on your surgical side when side lying.
Posterior Hip Precautions May Include:
Don’t bend your hip past a 90 degree angle.
Don’t cross your legs.
Don’t twist your hip inwards- keep knees and toes pointed upwards.
Adaptive Equipment
Once you meet with your Occupational Therapy practitioner, she/he will introduce something called a “hip kit”. A hip kit includes are a set of tools that will help you achieve your maximal level of independence while adhering to your hip precautions. These tools will help make your life a whole lot easier and help you avoid another trip to the doctor. In fact, the study done by Bozorgi et al (2016) concluded that patients who received rehabilitation services post hip replacement showed improvement. However, patients who were in the experimental group (which had additional supervision) and were trained in use of adaptive devices, demonstrated physical function, strength, reduced disability, and pain intensity significantly more than the group who weren’t trained on adaptive devices.
Hip Kits May Include:
A dressing stick
A sock aid
A reacher
A shoe horn
A long handled sponge
A bathroom bottom buddy
References:
Spalević, M., Milenković, S., Kocić, M., Stanković, I., Dimitrijević, L., Vesna Živković, V., Čolović, H., Spalević, M. (2018). Total Hip Replacement Rehabilitation: Results and Dilemmas. Acta Medica Medianae, 57(1), 48-53. doi:10.5633/amm.2018.0108
Lee, G. R. H., Berstock, J.R., Whitehouse, M. R., & Blom, A. W. (2017). Recall and Patient Perceptions of Hip Precautions 6 Weeks After Total Hip Arthroplasty. Acta Orthopaedica, 88(5), 496–499
Bozorgi, A. A., Ghamkhar, L., Kahlaee, A. H., & Sabouri, H. (2016). The Effectiveness of Occupational Therapy Supervised Usage of Adaptive Devices on Functional Outcomes and Independence after Total Hip Replacement in Iranian Elderly: A Randomized Controlled Trial. Occupational Therapy International, 23(1), 143–153.
With vaping being so popular these days a lot of young people are trying it. Vaping comes in different flavors, and this can be appealing to people because unlike a normal cigarette, which only comes in one flavor or taste, vaping seems to offer variety. However, with vaping being so new, the medical community does not know the full impact that it can cause on the body. Increasing reports are surfacing that show the damages that vaping can cause on the lungs.
I understand that vaping companies like Juul are marketed to help stop adults who are smoking. They should also be realizing what it is doing to teenagers. Teenagers are thinking that it is cool and posting videos on social media. They are not understanding that it is affecting their heath by getting them addicted to nicotine.
This is such a big problem for teenagers that even the President is stepping in. Companies need to start realizing the problem with vaping. They also need to start doing research on long term effects from vaping. In the next video, Trump mentions that people are dying from vaping. Just knowing this should turn a light bulb on in people’s heads and make them realize this is not safe.
With the public not knowing the full effects of vaping, people need to be careful with the product. If you haven’t started vaping, don’t start now just because people around you are vaping. It doesn’t mean it is safe. It took a while to find out what cigarettes can do to the body. Before jumping on board with this product, let’s figure out what is safe and what is not.
PANS/PANDAS is an autoimmune disease. What this means is when the body’s own immune system is activated from infection, in the case of PANDAS it is usually group A streptococci, and begins to not only attack the strep virus but the neurons in the basal ganglia. The basal ganglia is in control of voluntary motor movement, learning, eye movements, cognition, emotion and making choices that are construed as appropriate. When the basal ganglia is attacked by the immune system, the person exhibits certain symptoms. These symptoms are described by Murphy et al (2017) as obsessive compulsive disorder, and tic disorder, mood disorders, irritability, anxiety and what is term “rages”(p 640-641). Now, these symptoms taken by themselves usually appear to be psychiatric in nature. What separates the PANS/PANDAS patient is these symptoms occur suddenly after an infection, usually from strep. And they can be resolved with treatments that are not psychiatric. This short video explains the basics of the disease presentation.
The first step in treatment is recognizing that the patient has PANDAS. Again, sudden onset of symptoms after an infection is key. But how does someone know that there is an infection? A 24-hour throat and nasal swab culture is necessary, but these can come back negative because there are strep variants that do not show up on cultures. Another is the Cunningham panel blood test. This is a very specific blood test that looks for certain antibodies. The problem is not every hospital is able to provide this test. According to Leon et al (2018) the general course of treatment is, antibiotics that are effective against strep, along with anti-inflammatories (p 641). Also, some antidepressant and anti-anxiety medications. However, psychiatric medications should be minimal dose, as the patient symptoms are infectious in nature and not psychiatric. For long term maintenance Leon et al (2018) study shows that, intravenous immunoglobulin therapy (IVIG) and plasma pheresis can be considered and used to good effect (642). The problem is how to get these treatments to the patient.
What is the controversy?
Not every doctor, and insurance company believe that PANS/PANDAS is an actual
disease. Unfortunately, the popular media has portrayed PANS/PANDAS as a made-up disease for parents. Chicago Med on NBC Season 3 Episode 17 is such an example. This episode told the world PANDAS is a made-up disease given to parents by doctors to ease their worries. Also, insurance companies and government agencies have gone so far to take the position that PANDAS is not an actual condition. The Connecticut Insurance and Real Estate Committee has cited testimony from these anti-PANDAS agencies. These agencies state that due to the high cost of certain treatments coverage is not financially viable for insurance companies despite evidence that treatments are medically effective. In response, some states such as Illinois Department of Insurance, have put into law that PANDAS be covered by insurance companies.
The first step is to recognize your child has this condition. This can be done by seeing a specialist, usually an immunologist, that can make properly identify this diagnosis. There are certain tests that can be performed, The Cunningham panel was one previously mentioned. The second step is to see if the insurance company will pay for these tests and the subsequent treatments. Some insurances do provide services for PANDAS. But most do not and do not be surprised by this. Third step is to find out what treatments your doctor can provide. You doctor can still provide prescriptions for antibiotics, which are effective in reducing the symptoms. However, the most effective treatments are IVIG or plasma phereses. These treatments are usually not covered by insurance companies for PANS/PANDAS.
So what can you do if insurance will not provide coverage?
If you cannot get insurance to pay for treatments for PANDAS there are other possibilities. There are certain co-morbidities associated with PANDAS. A co-morbidity is a condition that is coupled with the first health issue. For instance, a person may have diabetes and a co-morbidity is heart disease. These PANDAS co-morbidities may be covered by the insurance company and can have the same treatments. A frequent co-morbidity of PANDAS is an immune deficiency such as common variable immune deficiency (CVID). Now another thing a person can do is look for an insurance company that does offer PANDAS treatment. This means doing research, finding an insurance company that offers treatment, and then finding an employer that uses that company. Finally, there is the option of paying for these treatments out of pocket. Be prepared for the high price because one treatment of IVIG costs approximately $10,000.00.
Trying to deal with PANDAS and get medical treatment is an exhausting and frustrating endeavor. There may be times, as a parent, you feel nothing can be done and it is hopeless to try and get treatment. That is a natural reaction and feeling. However, as difficult as it is to try and get treatment there is one thing to remember. Your child did not ask for this to happen to them, they did not ask for this disease and the stigma attached to it. Only person who will fight for them.
THAT IS YOU!!!
The parent is the greatest advocate for a child. Just remember that.
References
BIBLIOGRAPHY Ameratunga, R., Woon, S-T, Gillis, D, Koopmans, W, & Steele, R. (2013). New diagnostic criteria for common variable immune deficiency (CVID), which may assist with decisions to treat with intravenous or subcutaneous immunoglobulin. Clinical and Experimental Immunology, 174(2), 203-2011, doi: 10.1111/cei.12178.
Blake, K. (2016). AN ACT REQUIRING HEALTH INSURANCE COVERAGE FOR PEDIATRIC AUTOIMMUNE NEUROPSYCHIATRIC DISORDER ASSOCIATED WITH STREPTOCOCCAL INFECTIONS. Hartford: Connecticut Government.
Chicago Med, The Parent trap Season 3 Episdoe 17 (Season 3 Epsidoe). [Motion Picture].
Illinois Department of Insurance Fact Sheet PANDAS / PANS. (2019, Nov 8). Retrieved from Illinois insurance law: http://insurance.illinois.gov/HealthInsurance/Pandas-Pans.pdf
Kids suffer from debilitating episodes after recovering from strep throat (Nightline). (2019, Nov 10). Retrieved from Youtube: https://www.youtube.com/watch?v=N1D9xjSY5ns
Leon, J., Hommer, R., Grant, P., Farmer, C., D’Souza, P., Kessler, R., . . . Swedo, S. (2018). Longitudinal outcomes of children with pediatric autoimmune neuropsychiatric disorder associated with streptococcal infections (PANDAS). European Child & Adolescent Psychiatry, 637–643.
Molecular Labs. (2019, Nov 10). Grace’s Story: When strep triggers OCD, mood swings and behavioral changes. Retrieved from Youtube: https://www.youtube.com/watch?v=3VnHiCB8yFU
Murphy, T. K., Brennan, E. M., Johnco, C., Parker-Athill, E. C., Miladinovic, B., Storch, E. A., & Lewin, A. B. (2017). A double-blind randomized placebo-controlled pilot study of azithromycin in youth with acute-onset obsessive–compulsive disorder. Journal Of Child And Adolescent Psychopharmacology, 640-651.
PANS and PANDAS overview. (2019, Nov 11). Retrieved from Moleculera Labs: https://www.moleculeralabs.com/pans-and-pandas-overview/
Prelude: As a warning and for the reader’s knowledge this blog post is not driven by political or personal beliefs. This is to educate the public on current facts surrounding mental illness and gun violence. Is there a direct link?
I first came across this topic as the media continues to said that mental illness is a gateway to violence and mass shootings. I curiously started searching for statistics surrounding the subject. I personally thought to myself that maybe mental illness could increase violence. Then, I thought how I have struggled with mental illness; I thought about millions of people who suffer from mental illness and they do not kill people. Or do they?
Justine Coleman(2019) wrote a post for the Hill, an online news source. In her article she states that “Trump‘s administration is considering a proposal to study whether monitoring people with mental illnesses could prevent future violence, The Washington Post reported Monday”
Above we see a shot from a press conference by president Donald Trump. He is not the first administration to promise changes in mental health and gun laws. However, “According to Appelbaum,25 less than 3% to 5% of US crimes involve people with mental illness, and the percentages of crimes that involve guns are lower than the national average for persons not diagnosed with mental illness. Databases that track gun homicides, such as the National Center for Health Statistics, similarly show that fewer than 5% of the 120 000 gun-related killings in the United States between 2001 and 2010 were perpetrated by people diagnosed with mental illness” (Metzl & Macleish 2015 pg.2)
If less than 10% of crimes are directly related to mental illness then why do we associate people with mental illness as being more violent? It could be possible that we see people as “crazy” because of their abnormal behavior. Schizophrenia is a perfect example as people diagnosed may have hallucinations. In fact “more than 70%…” (Hugdahl et. al. 2008 pg.1) hear voices.
Anderson Cooper, a reporter for CNN, covered a story regarding schizophrenia that captures auditory hallucinations (hearing voices). He accurately experiences and reports honestly on his experience and opens up to the public. That we should not discriminate and we should help these people. You’ll find the link to this video below.
I wonder if the abnormal behavior we observe is what makes us assume they are violent. Therefore, we should educate the public including ours politicians and policy makers about what mental illness really is. Did you know that most severe mental illness leads people to isolate rather than go out? If a person is isolating themselves then how can they go out in public to hurt others?
Jessica Mcdonald (2019) said in her fact check article that “the National Council For Behavioral Health explained in its August 2019 report, “This means that if we could eliminate the elevated risk of violence that is attributable directly to having schizophrenia, bipolar disorder or major depression, the overall rate of violence in society would go down by only 4 percent; 96 percent of violent events would still occur, because they are caused by factors other than mental illness.”
Mass murder and gun violence and prevalent in the united states and in the world as we know it. Mass shootings are actually extremely rare in occurrence even though it feels like they are always happening. We as an international community need to break down stigma associated with mental illness. If mental illness causes only 4 percent of violence then why does the media say they cause so much violence?
Mass shootings are what drives the medias viewership. And a recent study by the Secret Service found that “between 2000-2013 found 25% of suspects had been diagnosed with a mental illness, and 62% had a mental health “stressor…” (Jessica Mcdonald 2019)
I feel as though if we educate out children on mental wellness and having a healthy mental well-being we can change the violence in our society. For centuries humans have fought wars and maintain a violent nature. However, if we start small, whether in a state or in a country we must educate our children and our public on mental illness to eliminate the stigma behind it.
References
Hugdahl, K., Løberg, E.-M., Specht, K., Steen, V. M., van Wageningen, H., & Jørgensen, H. A. (2008, March 28). Auditory hallucinations in schizophrenia: the role of cognitive, brain structural and genetic disturbances in the left temporal lobe. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2525988/
The flu shot dilemma… to vaccinate or not to vaccinate, has been an ongoing question for years. The media always has their own point of view and although we as people love to google everything and it is satisfying to have such quick access to information, we tend to read anything and obtain false information. Two great reliable sources for healthcare questions are the CDC and FDA. When it comes to vaccines, people should absolutely know all the facts about the vaccine they are about to receive. It is important to check a credible site or watch a credible source of a video. One credible source is your PCP (primary care physician). When you go to your wellness visit or you want to inquire about the flu shot, your PCP will be able to provide a print out of reliable information regarding the facts about the vaccine.
We as consumers and patients are faced with many questions-
Who should get the flu shot? Everyone from the ages of six months and older.
Why should we get the flu shot? Because one prick could keep you from missing weeks of work (or worse). The flu vaccine is never 100 percent effective, but “it still prevents millions of illnesses and deaths each year,” says William Schaffner, MD, an infectious-disease expert at Vanderbilt University. “Even if you do get sick, your symptoms are likely to be milder.” The shot also slashes your odds of passing the virus to babies, the elderly, and anyone with a compromised immune system (like a cancer patient).
When should I get the flu shot? Late September or early October. The vaccine is usually available as early as August—but because it’s only effective for about six to seven months, waiting until fall officially begins can ensure you have coverage through the end of flu season (which is typically late April). Though you may have heard otherwise, you don’t have to get a vaccine twice in a single season: “Just wait until fall so you’re protected for the next six months,” says Dr. Schaffner.
Will I get sick after I get the flu shot? Getting sick after the shot is just a myth. There are any other viruses that you may contract during the period of getting the flu shot.
Does it hurt? The site will be slightly sore for a day or so following injection. reactions vary from individual to individual.
Down below will be a video that separates the facts from fiction about the flu shot dilemma.
This media clip actually states the same facts that my referenced articles do so this is a factual writing for me. The facts from the articles will be provided below.
Ways to “Boost” your immune system
warm up in a sauna
break a sweat most days (exercise regularly)
go to bed early
eat healthy
get a massage
If you have a strong immune system, the chances of you contracting a very bad illness such as the flu, are slimmer than someone who has a very low immune system. Even if you do get sick, you will recover quicker and not be as severely sick then if someone has a poor immune system. Complications from flu can be severe and usually require hospitalization. Complications arising from flu include: • Viral pneumonia. • Secondary bacterial or viral infections. • Multi-organ failure. • Rarely: encephalopathy, myocarditis, transverse myelitis, pericarditis and Reye’s Syndrome. • Worsening of chronic illnesses, especially in those with metabolic, pulmonary and cardiac conditions.
Your age and state of health also play a role in determining how well the flu shot will protect you. As we age, our immune systems are much weaker. We may not produce as many antibodies to the virus in the vaccine as they did when we were younger. Even if the vaccine is a perfect match, we may not generate an immune response strong enough to fight the virus off. Several illnesses and medications can also dampen your immune response.
A study done over three years showed that flu-related hospitalizations decreased by 61% in people over 50 years who had received the flu vaccine. It is important to note that delaying flu vaccination in the elderly in order to provide better immunity later in the flu season, may result in losing the opportunity to vaccinate and also having a larger volume of people to vaccinate within a limited time period.
So, in conclusion it is safe to say that it is an important topic of the community and the flu shot does play a huge role in quicker recovery and education is key to the public.
References:
Pag, n, C. N. (2018). Prep for Flu Season Now! Health, 32(7), 73–76. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=131109430&site=ehost-live
Surviving the flu season. (2016). Harvard Women’s Health Watch, 24(4), 1–7. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=119520627&site=ehost-live
What is autism, really? There is a lot of misconception about people with autism. Are they a different species of humanity? To debunk these myths, here are various peer-reviewed resources to clarify these misconceptions:
Peer-Reviewed Source No. 1: Raff, 2010
To start, Autism Spectrum Disorder or ASD is a spectrum, and probably the reason for the apparent increase in the diagnostic criteria of Autism as it has expanded enormously.
Three Functional Levels of Autism:
Level 1, which is regarded as high functioning autism, are Asperger kids, who have much less trouble with language.
Level 2, the spectrum in the middle, in which patients may need substantial support.
Level 3,which is considered Severe Autism, is the most challenging end of the spectrum. The patient’s social, communication, and repetitive behaviors severely impair daily life activities.
The defining features of autism are the three core features, such as:
the problem with social interactions, which is often the heart of the matter, a problem with language,
a tendency to have restricted interests and
repeated stereotypic motor behaviors.
These are the so-called autistic triad, and you need to have two of the three and to develop them by the age of 3 to be considered autistic.
This media clip portrays real ASD patients in three different levels:
Peer-Reviewed Source No. 2: Elder Robison, 2018
Just like in the article “What is Autism” by John Elder Robison, the author talks about his struggle and point of view about his autism. Robison’s (2018) work of literature supports the media clip “Just Like You – Autism.” The author clarifies that his experience of the world is just as valid as anyone else’s. When he associates colors with sounds or see details others can’t, his knowledge of those things is just richer than that of others. The author calls this as a gift. He explains that when nonautistic people look at a machine and sees a problem that is impossible to understand, that too is a gift. This back-up the information in the media thatpeople with autism are just like anyone else but different.Just like the media clip I choose, it talks about children with autism who are the same as other kids but different in their own ways.
This literature also supports the information in the media that people with autism require assistance, such as making friends and integrating into society. People with ASD ask for help communicating, and when medicine can’t provide answers, they turn to engineers. Now, formerly nonspeaking autistics are finding a voice through electronic technology and assistive devices.
This research is about young children with Autism Spectrum Disorders (ASD), demonstrating fewer and less varied play behaviors than children with typical development. The study has shown that children with ASD do not engage in the same levels of spontaneous play as children without disabilities, even when matched for mental age and receptive and expressive language abilities. This research supports the information in the media clip from the service provider Autism Queensland,in which the child wasn’t responding to his name when he was a baby, didn’t play peek-a-boo, or won’t play with the grandmother or anyone else but himself.
This literature explains that play is a primary context for participation for young children with disabilities in early childhood settings.
Play skills contribute to children’s
social,
cognitive and
language development
So based on the media clip, since the baby wasn’t participating in play, it affects his social and language development as well. Early Intervention, additional support, and further assistance that the child needs, as stated in the video, are essential for him to develop these skills.
According to my research, the media clips I choose got the facts right and provided clarity and specificity about autism. The viewers of these media clips can feel confident that he or she has been offered correct medical information on the truth about autism.
References
Barton, E., Gossett, S., Waters, M. C., Murray, R., & Francis, R. (2019). Increasing Play Complexity in a Young Child With Autism. Focus on Autism & Other Developmental Disabilities, 34(2), 81–90. https://doi.org/10.1177/1088357618800493