3d Bipolar disorder background
Bipolar disorder throughout the years has gained a bad reputation through media like TV shows or the internet. They use the word “bipolar” as a generic label for someone who is being moody or unreasonable. There are many myths created that need to be looked at and determine whether it is fact or fiction. Three statements I hear constantly is” being bipolar is a character flaw, “They’re just crazy” and “There is no cure”. Bipolar disorder is a mood disorder that deals with a certain part of the brain. This part of the brain is in charge of making decisions, judgment, and moods. The commonly used definition of this disorder is mood swings involving times of depression alternating with periods of euphoria (extreme excitement & happiness). Sometimes they can become extremely energetic then become severely irritation. These intense mood swings are commonly known as the manic phases of bipolar disorder. Most may experience more than one episode of these dramatic mood changes. With this disorder, it is not a constant “mania”. There can be a long period of time in between these episodes without any problems.

Fact or myth?
Having bipolar is a character flaw: MYTH
You can’t choose to be bipolar. You also can’t just turn it off and get yourself together. It is not a figment of imagination. It is a real disorder that takes place in the brain. It is still not completely understood how or why it happens. It is strongly suggested to be linked to genetics (DNA). Head trauma and extreme stress are risks that may lead to bipolar disorder usually if already genetically linked.
Having bipolar means you’re always crazy: MYTH
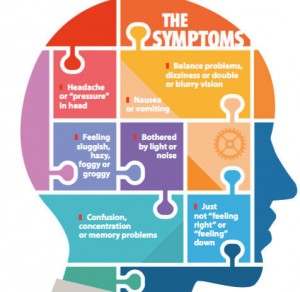
People can experience a series of highs and lows with times in between that can last months to years with no mood swings. They are not in a constant mania, all the time. Some signs and symptoms of this disorder includes fast talking & topic jumping, lack of sleep, increased sex-drive, extreme happiness, over confidence, meddling, irritation, defensive, depression, anxiousness, suicidal thoughts. Looking over the list you can see there are a number of different moods one may go through during a manic episode. They are not “crazy”.
There is no cure for Bipolar disorder: MYTH
Medication can help stable moods and decrease episodes. It may take a few different trials of medication to individualize the best treatment. Talking with a therapist may help with other issues the individual may be experiencing. Support groups and psychotherapy could also help. Hospitalization may result in severe cases.
There are a number of people who do not understand what bipolar disorder really is or what it’s like to live with the disorder for the rest of their lives. Media gives bipolar a bad rep but is now becoming more recognized by TV shows portraying the difficulties one with bipolar suffers from. It is one thing to read and become educated on this disease but it is another if you know what it feels like to go through it. Ones who suffer from this disorder are not “crazy” or “unmanageable”. With support and therapy, a normal lifestyle can be maintained.
More information on facts and myths about Bipolar Disorder
http://www.heretohelp.bc.ca/factsheet/bipolar-disorder-myths-and-facts
References
Astrês Fernandes, M., Jardel Feitosa Sousa, K. H., Aprígio de Andrade, P. C., Soares de Carvalho, L. C., Dias Pereira, D. B., & Melo Silva, B. J. (2016). BIPOLAR AFFECTIVE DISORDER, CURRENT MANIC EPISODE WITH SYMPTOMS OF PSYCHOTIC AND CARE IN NURSING. Journal Of Nursing UFPE / Revista De Enfermagem UFPE, 10(2), 669-674. doi:10.5205/reuol.8557-74661-1-SM100220163
Janicak, P. G., & Esposito, J. (2015). An Update on the Diagnosis and Treatment of Bipolar Disorder, Part 1: Mania. Psychiatric Times, 32(11), 29-34.
Sullivan, R. J., & Sullivan, S. (2016). AN EMS GUIDE TO DEPRESSION AND BIPOLAR DISORDER…republished from the EMS Reference. EMS World, 45(6), 48-56.