While the internet is a great resource to find and learn information about anything you could imagine, it also contains information that is incorrect. Emergency contraception pills (ECPs) are one of the topics that is surrounded by rumors and misunderstandings. Even though ECPs have been studied for over 50 years by medical professionals, people still tend to believe the rumors this medication.
So what exactly is emergency contraception pills (EPCs) and when would I need to use them? ECPs is an effective contraceptive method that is used to reduce the risk of unwanted pregnancy after unprotected sex or contraceptive failure (Bauzà-Amengual, Esteva, Ingla-Pol, Font-Oliver, & March, 2018). According to Planned Parenthood, the levonorgestrel morning-after pill like Plan B can lower a woman’s chance of getting pregnant by 75-89% if it is taken within 3 days after unprotected sex or contraceptive failure. Other factors that affect the effectiveness of ECPs include a woman’s body mass index (BMI) and the length of time the EPC is taken. Having a higher BMI makes EPCs less effective.
Below is a video that was aired by Fox News in 2013. The doctor and the new anchor are discussing ECPs and how the age limit has changed over the years. The title of the video includes false infomation about ECPs.
So first we’ll discuss the misconceptions or myths. The biggest misconception surrounding ECPs in that they cause abortions. Now let’s talk fact. EMERGENCY CONTRACEPTION PILLS DO NOT CAUSE ABORTION. ECPs work by delaying ovulation. Meaning the egg and sperm do not make contact which prevents a pregnancy from developing. The medication that is used in most ECPs, Levonorgestrel, has absolutely no effect on an established pregnancy. This means if a woman is already pregnant and takes ECP it will not be effective and the pregnancy will continue to develop.
Another myth is that there is only one ECP option and that it is hard to get. This is simply not true. Like anything in this world, there is a competition of products from different companies. There are more than two dozen different types of ECPs available in the United States. The most well known ECP is Plan B One-Step and the generic versions like Next Choice One Dose, My Way, and Take Action. EPCs are available in pharmacies, in stores, and online without a prescription or age restrictions. Most clinics accept walk-in patients as well.
A third misconception surrounding EPCs is that taking too much affect your fertility. There is zero evidence that taking ECPs multiple times with affect future fertility of a woman. The only side effects of ECPs include upset stomach, feeling lightheaded or dizzy, having tender breasts for a short while after a woman takes the pill, and the woman’s next period could potentially be heavier or different from the woman’s normal period. Another potential side effect is nausea or throwing up. An important thing to know is that if a woman throws up within 2 hours of taking the pill, it will not be effective and they should retake the medication.
ECPs are an option for women who have unprotected sex or if their birth control method fails. It does not cause abortions and it does not affect a woman’s fertility. The internet is full of information but it is important to look further and learn the absolute truth.
References
Bauzà-Amengual, M. L., Esteva, M., Ingla-Pol, M., Font-Oliver, M. A., & March, S. (2018). Discourses on the postcoital pill in young women. BMC Public Health, 18(1), N.PAG. https://library.neit.edu:2404/10.1186/s12889-018-5691-3
In present day there are many people being diagnosed with diabetes or are unable to keep it under control, especially type I or uncontrolled type II diabetics, this is when insulin is introduced to their daily medication regimen. With the use of insulin the body attempts to learn how to maintain your blood sugar within 70-140. Although with insulin therapy hypoglycemia can occur as a side effect. Hypoglycemia in diabetics is defined as a blood sugar <70 with or without symptoms, which can expose someone to harm (Brackney, 2018). To prevent this from occurring, monitoring blood sugar levels is crucial, knowing and recognizing signs or symptoms, as well as knowing what to do in the case that this does occur.
Signs and Symptoms
Palpitations
Sweating
Anxiety
Hunger
Nausea
Tingling
Trembling
Difficulty concentrating
Headache
Dizziness
Vision change
Weakness
Drowsiness
Severe symptoms (Usually with a blood sugar <40)
Coma
Confusion
Seizures
(Leung, 2018).
Treatment
The treatment or intervention is based on the person’s condition; whether they are alert, able to swallow, unconscious and what setting they are in. In this blog, it is based off a home setting.
It is important to carry a carbohydrate at all times. In the case that this does occur a carbohydrate or a drink with sugar should be ingested and re-check your blood sugar in 15 min and continue to do this until your blood sugar is above 70. It is also recommended to carry glucagon, which a family member can administer intramuscularly in case of an emergency, and if the patient is unconscious. Not merely is education important for the person with diabetes, but also for ones family members.
Mild Hypoglycemia
Three to four glucose tablets;
4 to 6 oz fruit juice or regular soft drink;
6 oz regular soda (not sugar-free);
8 oz (1 cup) sports drink (not sugar-free);
1 T sugar or five small sugar cubes; or
1 T syrup or honey.
(Weiner, 2017).
Severe symptoms of hypoglycemia
Family members can call 911
Glucagon intramuscularly
A video is provided below about how to treat hypoglycemia
Prevention
Frequent blood sugar monitoring
Exercise/diet
Follow the instructions given by your primary care physician or endocrinologist
Carry a carbohydrate snack or orange juice
Carry glucagon incase of an emergency
Administer insulin as prescribed
References
Brackney, D. E. (2018). Hypoglycemia: An unwelcome companion to effective diabetes management. American Nurse Today, 13(8), 6–13. Retrieved from http://library.neit.edu:2084/login.aspx?direct=true&db=ccm&AN=131145487&site=ehost-live
Leung, E. (2018). New and Not so New Information on Hypoglycemia and Prevention Strategies. OOHNA Journal, 37(1), 20–22. Retrieved from http://library.neit.edu:2084/login.aspx?direct=true&db=ccm&AN=132938311&site=ehost-live
Weiner, S. (2017). Hypoglycemia Prevention and Management. Today’s Dietitian, 19(7), 36–39. Retrieved from http://library.neit.edu:2084/login.aspx?direct=true&db=ccm&AN=124137905&site=ehost-live
The argument for the benefits of vaccines has been a long fought battle. With the rising trending of autism diagnosis has lead to many parents and researcher to come to the conclusion that there must be a definite cause to this trend.Opposition to vaccines as a whole has always been around. A more recent argument against vaccines is the theory that believes the MMR is responsible for causing the increase in the cases of Autism today despite there being no medical or biological studies that prove this theory.Majority of the research discredits and contradicts the argument against Vaccination
Arguments Made by this video
Vaccines are responsible for children being diagnosed with autism.
An infant natural immunity is better than obtaining acquired immunity through vaccines.
Vaccines can actually cause the child to contract diseases it designed to protect against.
Max production of Vaccines made lead to error in concentration and contents of each vaccine batch.
Vaccines are considered obsolete due to the low rates of infection rates in America.
Describes the increase in a move against vaccination. One of the main concerns is that the consistent decrease in vaccination will eventually lead to a large epidemic.
Points out the false nature of Wakefield’s paper which is responsible for initial connection between the MMR vaccine and autism
Advocates for simple platforms that parents can learn about factually information about the MMR Vaccine.
Speaks on the possible dangers of the Anti-Vaccination movement.
Speaks on increase in deaths linked to decreased vaccinations.
Describes Common fears about MMR Vaccines
Peer Reviewed Sources
Source # 1
Offit & Gerber 2010, aim to explore 1) whether or not the combination of MMR vaccine causes damage to the intestinal lining, which provides opportunity for encephalopathic proteins to enter and cause damage, 2) the MMR vaccine contains preservatives that are toxic to the Central nervous system, 3) providing multiple vaccines overload the weak infant immune system. The researcher made use of several ecological based studies to evaluate 498 Autistic children born from 1972 to 2002. Offit & Gerber 2010, looked into completing a time trend analysis to explore the trend in vaccination and medical records of children diagnosed with autism.Overall the researcher found there were was no direct cause correlation between thimerosal and autism.
Offit & Gerber 2010 discovered that there was no direct correlation between the vaccines and the immunes system of the child being overworked. Offit & Gerber 2010 discovered that vaccines are minute in comparison to the danger that infants face on a daily basis when fighting off various diseases and infections. Additionally, Offit & Gerber 2010 was able to come to the conclusion that there is no significant difference in infection susceptibility between vaccinated and non-vaccinated children.
Source 2
Miller et al 2003, put forth the idea that the concern of providing infants with the combined MMR vaccine warrants any serious concerns. Miller et al 2003, explored the notion that children provided the MMR vaccine would exhibit significant immunosuppression post-vaccination period. Miller at al 2003 , utilized the cases of bacterial infection and pneumonia in children 1-2 years who were hospitalized between April 1991 and March 1995. Miller et al 2003, utilize ICD codes to locate infections in infants after a 12-week wait period. The children were compared to a control group. After reviewing the case Miller el al 2003, concluded that there was no direct correlation between the MMR vaccine and infections post-vaccination period. Overall Miller et al 2003, suggested that this danger of MMR vaccine being further explored.
Source 3
The rising support for Anti-vaccine movement has lead to numerous parents refusing to vaccinate their children due to fears of infection, disease and “contracting” autism. As a result of the phenomenon, there has been a measles outbreak in many western countries where measles was not normally seen. Hussain et al 2018, set out to explore how the movement started, and how the repercussions of the movement have affected public health and safety.
The Anti-vaccination movement originated from the early England religious movement against many medical processes, which were deemed “Diabolic operations”. Andrew Wakefield who published the Lancet, which renew the theory that was was a correlation between autism and the MMR vaccine. His study was discredited due to monetary complication and he was forced to retract his statement. Unfortunately, his findings were already spread and began to influence many parts of the world. As a result, the MMR vaccination rate dropped in London, Ireland, and the US. The resulting outbreaks lead to several child deaths and a strain of the healthcare system.
References
Gerber, J., & Offit, P. (2009). Vaccines and Autism: A Tale of Shifting Hypotheses. Clinical Infectious Diseases,48(4), 456-461. doi:10.1086/596476
Hussain, A., Ali, S., Ahmed, M., & Hussain, S. (2018). The Anti-vaccination Movement: A Regression in Modern Medicine. Cureus. doi:10.7759/cureus.2919
Miller, E. (2003). Bacterial infections, immune overload, and MMR vaccine. Archives of Disease in Childhood,88(3), 222-223. doi:10.1136/adc.88.3.222
WhatsGoingOn, T. (2015, August 19). Retrieved February 06, 2019, from https://www.youtube.com/watch?v=mTjvX6s2Jvk
We have all heard the instructions, perhaps barked at us as we are reaching for that after school snack as a child: WASH YOUR HAND FIRST! As adults we may not have someone reminding us, but the duty to wash our hands remains the same. In order to stay healthy and continue to attend to our families, jobs, and social life, we must do our best to prevent the spread of bacteria and viruses that can make us sick.
According to Adane, et al. (2018) the critical points to wash your hands include after using a restroom or changing a small child, before eating, feeding a child or preparing food. These crucial times offer the opportunity for bacteria in our environment to enter the body to cause illness. Most illness is caused from a bacteria spread via fecal oral route, and this tiny bacteria that spreads from you-know-where is completely invisible to the naked eye–but can be removed by hand washing.
If you feel crunched for time, you are not alone. In fact, Chittleborough et al (2012) found that this was the biggest reason for students and faculty to cut the handwashing scene short. In reality, the recommended time for handwashing is the amount of time it takes you to sing “happy birthday” to yourself two times. In hand sight, singing a song we all know by heart a couple of times seems like a small price to pay in order to stay healthy.
References
Adane, M., Mengistie, B., Mulat, W., Medhin, G., & Kloos, H. (2018). The Most Important Recommended Times of Hand Washing with Soap and Water in Preventing the Occurrence of Acute Diarrhea Among Children Under Five Years of Age in Slums of Addis Ababa, Ethiopia. Journal of Community Health, 43(2), 400–405. https://library.neit.edu:2404/10.1007/s10900-017-0437-1
Chittleborough, C. R., Nicholson, A. L., Basker, E., Bell, S., & Campbell, R. (2012). Factors influencing hand washing behaviour in primary schools: process evaluation within a randomized controlled trial. Health Education Research, 27(6), 1055–1068.
Opioids, also known as narcotics, are medications prescribed by doctors to treat persistent or severe pain. Some common types of Opioids are known as Codeine, Fentanyl, Oxycodone, and Morphine. Opioids were originally created for the purpose of pain management but have been known to be abused. In the 1990’s there was a massive marketing scheme from pharmaceutical companies for their new opioid pills. This coincided with a nationwide push to take patient pain more seriously. “In 2015, more than 33,000 Americans died as a result of an opioid overdose and an estimated 2 million people in the United States suffered from substance use disorders. Opioid overdoses increased 30 percent from July 2016 through September 2017 in 52 areas in 45 states” (National Institute on Drug Abuse, 2019). Opioid abuse has resulted to be a difficult and complex problem.
Opioids are prescribed by a doctor to minimize one’s pain from trauma, post-operative pain, acute illness, fractures, etc. These are all examples of acute pain; which lasts a few days to a week. Doctors have advised that during that particular time frame is when individuals should be prescribed narcotics and after that week, the person is recommended to take over the counter medications to alleviate any other discomfort they may experience. Despite the fact that doctors have been given certain guidelines to follow, some tend to ignore the recommendations and thus leads to increased risk for their patients.
Along with this, society has placed the majority of the blame on doctors due to their lack of knowledge and education. A physician stated ‘“In medical school we were always told not to under treat pain in patients and that patients don’t become addicted to opioids when they really have pain”’ (Hubbard, Hodge Jr., & Rempel, 2018, p.169). Issuing the prescriptions writes off the patient but the patient then writes a satisfied survey, creating good results for the doctor. “After all dispensing prescriptions has become so commonplace that patients expect to obtain medication orders as part of a standard medical visit and they may leave the office dissatisfied if this expectation is not fulfilled” (Hubbard, Hodge Jr., & Rempel, 2018, p.169). As a result, opioids have become an overprescribed problem throughout the nation along with its serious side effects/consequences to the patient.
References
Hubbard, J., Hodge, S. D., & Rempel, R. (2018). Opioid Abuse: The Fall of a Prince. Quinnipiac Health Law Journal, 21(2), 159–202. Retrieved from http://library.neit.edu:2048/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=lgs&AN=132837820&site=ehost-live
First, let me explain what Carpal Tunnel Syndrome (CTS) is before I continue with CTR. It is the condition where the median nerve is entrapped in the tunnel space that it shares with nine flexor tendons. Above this tunnel space is the transverse carpal ligament.
When this tunnel space swells up, the median nerve can be pressed against the flexor tendons, the transverse carpal ligament, and the tunnel space. When this occurs, numbness, tingling, and pain may occur in the hand that shoots up to the thumb, index finger, long finger, and half of the ring finger. This can be due to a variety of reasons which include: fractures, swelling during pregnancy, arthritis, thyroid conditions, as well as job-related tasks such as a baker, a cashier, a farmer, a mechanic, a gardener, a musician, a front office assistant (using computer all shift), and many more jobs that require the frequent repetitive use of the hands.
After tests are completed and a diagnosis for CTS is done, all conservative treatment (non-surgical) will be attempted first with surgery as the last resort. Some conservative treatments include:
Changing patterns of hand use to reduce pressure
Keeping the wrist splinted in a straight position to reduce pressure
Wearing wrist splints at night to relieve symptoms that interfere with sleep
Steroid injections into the carpal tunnel to reduce swelling
Outpatient Physical Therapy or Occupational Therapy can help reduce pain levels
If these treatment options do not work, then the physician would talk to the client about choosing surgery to relieve the pain and discomfort.
According to Atroshi, et al, surgery for CTS is one of the most performed procedures being done in the U.S. with 350,000 procedures performed annually. The largest proportion are done amongst the working adult and more often amongst women.
This surgery is done on the outside of the skin in order to make an incision inwards to cut the transverse carpal ligament to relieve pressure placed on the median nerve. According to University of Michigan, cutting the base of the palm of the hand involved with CTS helps the doctor to see the transverse carpal ligament. It is done with local anesthesia, stitches after surgery, and the client gets to go home the same day.
***Be aware this video contains graphic images of surgery being performed***
What is Endoscopic Carpal Tunnel Surgery for CTS?
This type of surgery is done using a thin tube with a camera attached. The endoscope will help guide the surgeon through the small incision made on the wrist. The cutting tools for this type of surgery are tiny and will also be inserted along side the endoscope. When the transverse carpal ligament is found, the cutting tool will be used to make cut this ligament freeing the median nerve from pressure.
***Be aware this video contains graphic images of surgery being performed***
The question is: which type of surgery would be better for the patient with CTS?
I currently work at an outpatient Physical Therapy clinic, and most (if not all) of my clients had the Open Release done for CTR surgery. I had only seen one Endoscopic Release client, but it was at my prior job. From my experience treating these two post-operations (post-op) for therapy, it appears that the clients I had worked with who had the open release done had more pain and discomfort than the one I had seen with the endoscopic release.
Aforementioned earlier in this blog, CTS symptoms usually occur amongst adults – more frequently among the working adult population. In this case, many working adults who are highly recommended to have surgery done will want to go back to work immediately or as soon as possible. However, this invasive surgery takes time when it comes to the healing process. It is dependent on the individual on how quickly the hand will heal. I have observed an elderly woman in her 90s who had CTR done with the open release option, who had no pain and was able to function normally after several days post-op. Then I remember vividly a teacher who I had worked with in her late 40s who also had the open release surgery done, but it took 4-6 months for the intense pain to subside. She had what was known as pillar pain. In regards to pillar pain, the client I worked with who had endoscopic surgery done did not experience pillar pain.
According to Feller, et al. pillar pain “is a known complication following carpal tunnel release and can be debilitating, causing a decrease in strength and delayed return to work/recreational activities. It is defined as pain and tenderness localized to the prominences of the trapezial ridge, scaphoid tubercle, pisiform or hook of the hamate.”
When planning for CTR surgery, the clients should be given all treatment options for consideration, especially these two options. Expert surgeons continue to debate about carpal tunnel syndrome treatment and the following are their reasoning.
Pro Open Release
Traditional open carpal tunnel release (CTR) gives surgeons full visualization of the hand structures, which may decrease the risk for nerve damage. The trade-off: increased sensitivity.
“Overall, I think that the incidence of complications for an open carpal tunnel release done in experienced hands is very low,” said Simmons, who is also an Orthopedics Today editorial board member. “[It is] probably in the 0.02% complication rate, meaning nerve injury. But, the major thing is the tenderness in the palm.”
Pro Endoscopic Release
James Chow, MD, who is president of the Arthroscopy Association of North America (AANA) and developer of the Chow technique, explained the reasoning behind the benefits of endoscopic release. He states the following:
Endoscopic carpal tunnel release has three purposes: preserve normal anatomical structures, increase safety and avoid serious complications. However, critics of endoscopic surgery state that there is short-term benefits and has increase complications to this surgical option. “This is a misconception. Let’s ask ourselves a few questions. First, what is the fundamental difference between endoscopic and open carpal ligament release?” he said. “The open surgery cuts from the outside in, and the endoscopic procedure cuts from the inside out. Next, where are the important structures? Are they inside the carpal canal or outside the carpal canal? Then ask yourself, which is safer: To cut it before you see it or to see it before you cut it?
STUDY DONE OF CTR SURGERY: Open Release vs Endoscopic Release
Another article that I found had completed a study to compare both the open release surgery and endoscopic release surgery and post-op conditions regarding pain, sensations, and functionality to go back to work. The study appear to back up the information that Dr. Chow described aforementioned. In this study, 128 employed clients ranging from 25-60 years old were clinically diagnosed and electrophysiologically confirmed with idiopathic carpal tunnel syndrome.
Main outcome measures: The primary outcome that were being observed was the severity of post-operative pain in the scar or proximal palm and the degree to which pain or tenderness limits activities, each rated on a 4 point scale, transformed into a combined score of 0 (none) to 100 (severe pain or tenderness causing severe activity limitation). The secondary outcomes were length of post-operative work absence, severity of symptoms of carpal tunnel syndrome and functional status scores, SF-12 quality of life score, and hand sensation and strength (blinded examiner); follow-up at three and six weeks and three and 12 months.
Results: There were 63 patients who had undergone endoscopic surgery and 65 patients who had open surgery, with no withdrawals or dropouts. Pain in the scar or proximal palm was less prevalent or severe after endoscopic surgery than after open surgery, but the differences were generally small. At three months, pain in the scar or palm was reported by 33 patients (52%) in the endoscopic group and 53 patients (82%) in the open group (number needed to treat 3.4, 95% confidence interval 2.3 to 7.7) and the mean score difference for severity of pain in scar or palm and limitation of activity was 13.3 (5.3 to 21.3). The median length of work absence after surgery was 28 days in both groups. Quality of life measures improved substantially.
Conclusions: In carpal tunnel syndrome, endoscopic surgery was associated with less postoperative pain than open surgery, but the small size of the benefit and similarity in other outcomes make its cost effectiveness uncertain.
Healthwise Staff. (2017). Endoscopic Carpal Tunnel Surgery for Carpal Tunnel Syndrome. Cigna International. Retrieved: May 8, 2019. <https://www.cigna.com/individuals-families/health-wellness/hw/medical-topics/endoscopic-carpal-tunnel-surgery-for-carpal-tunnel-hw212492>.
CCOHS. (2014). Carpal Tunnel Syndrome. Canadian Centre for Occupational Health and Safety. Government of Canada. Retrieved: May 8, 2019. <https://www.ccohs.ca/oshanswers/diseases/carpal.html>.
Healio. (2006). Expert surgeons continue the heated debate about carpal tunnel syndrome treatment. Orthopedics today. Retrieved: May 8, 2019. <https://www.healio.com/orthopedics/hand-wrist/news/online/%7B576e9ea9-2568-4420-bd11-3df553434589%7D/expert-surgeons-continue-the-heated-debate-about-carpal-tunnel-syndrome-treatment>.
Healthwise Staff. (2018). Open Carpal Tunnel Surgery for Carpal Tunnel Syndrome. Michigan Medicine. University of Michigan. Retrieved: May 8, 2019. <https://www.uofmhealth.org/health-library/hw212359#hw212359-Bib>.
ASSH. (2015). Carpal Tunnel Syndrome. American Society for Surgery of the Hand. Retrieved: May 8, 2019. <https://www.assh.org/LinkClick.aspx?fileticket=7ToQme1rt_k%3D&portalid=1>.
Feller, et al. (2017). Prospective Evaluation of Patients Undergoing Carpal Tunnel Release and the Development of Pillar Pain. Department of Orthopaedic Surgery, Warren Alpert School of Medicine, Brown University, Providence, RI. Retrieved: May 8, 2019. <https://www.ors.org/Transactions/63/2117.pdf>.
Atroshi, et al. (2006). Outcomes of endoscopic surgery compared with open surgery for carpal tunnel syndrome among employed patients: randomised controlled trial. US National of Library of Medicine National Institute of Health. NCBI. Retrieved: May 8, 2019. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1482334/>.
Dacus, et al. (2014). Open Carpal Tunnel Release – Dr. Dacus. UVA Hand Center. University of Virginia School of Medicine. Retrieved: May 8, 2019. <https://www.youtube.com/watch?v=HgjpjSGhzt8>.
Even though the opioid epidemic was declared a public health emergency on October 16, 2017 by the US Government, opioids have been a problem since the 1990’s. It has gotten progressively worse as more and more patients are being prescribed opioids for every category of pain even if it’s not warranted. The issue with patients being addicted to opioids is that they are at a higher risk for addiction to other deadly street drugs such as heroine and methamphetamine.
Massachusetts has the highest number of opioid related deaths in the US and the highest prescribing rates of opioids are in Boston.
Categories of Pain
There are many different subcategories of pain, but the three main categories are Acute Pain, Chronic Pain, and Neuropathic Pain.
Acute pain is short lived and usually only lasts for 3 to 6 months. Acute pain can be a result of tissue damage and/or injury. Chronic pain lasts longer than 6 months. Chronic pain can be a result of an underlying injury with or without an underlying condition. Neuropathic pain is more of a nerve pain, its felt as a tingling, burning, stabbing pain that can travel down the body. Neuropathic pain can be either acute or chronic depending on the condition.
Prevention
The issue with pain management is that pain is subjective to every patient. There is no true set medical procedure or test to assess the patient’s severity of pain. Healthcare professionals perform pain assessments, but they are subjective and a patient can say their pain is a 10/10 while they were sleeping prior to coming in to see them. It’s hard to differentiate and cases severe backlash from patients to question their pain level. Proper health screenings and assessments need to be completed by the patient’s physician to see what category of pain the patient is experiencing and what the best type of pain management is appropriate for the patient.
Different Types of Opioids
There are short and long acting opioids. The 5 main categories of opioids are:
-Hydrocodone (most commonly prescribed opioid in the US)
-Oxycodone (most commonly found in tablet or pill form)
-Codeine (most commonly prescribed as a cough syrup)
Since opioid are so highly addictive and gaining more and more popularity in the streets, different tools can help physicians decipher if opioids are the proper management for the patient’s pain.
-Urine drug screen can be performed on patients that seem like they are “pill-seeking” or “doctor/hospital shopping”. This is a tricky slope, patients can become very insulted and or agitated if they are questioned on their addiction, especially if they are abusing drugs. Certain physicians and hospitals have a protocol to drug screen every patient regardless of background or condition.
-Risk-assessment tools can be utilized to help physicians decipher if a patient is at a higher risk for opioid addiction and if opioids are the proper treatment plan.
-Prescription drug monitoring programs and National All Schedules Prescription Electronic Reporting Act is a database that physicians can utilize to plug in a patient’s name to see if the patient if a “frequent flier” or “doctor or hospital shopping”.
Treatment Options for Opioid Addiction
The government has increased their resources for improved and more availability of opioid rehabilitation and treatment centers. The government has also made it easier for patients to be accepted into these programs regardless of health insurances.
Other medications can be prescribed for pain management while the patient is recovering from addiction, such as:
-Anti-inflammatory drugs
-Antidepressants
-Antiepileptics
-Nerve Blocks
Also, there are medications that can be given specifically for opioid addiction:
-Methadone
-Buprenorphine
Naltrexone
The media does portray these types of medications in a poor light because they want the population to believe that the healthcare world is just changing one drug for another drug that the government can regulate and get money for.
-The population is unaware that opioid addiction is a highly treatable illness.
-Nonfatal opioid overdose is a reversible condition, meaning a patient can be treated for it.
-There is not enough studies or tests performed on chronic pain patients, to see if opioids are truly the best option for this patients.
-The longer a patient stays on opioids the higher the dose they will continue to need to have their pain managed.
-Opioid addiction comes with multiple other side effects such as constipation, nausea, decreased sex drive, increased sensitivity to pain.
-Opioid epidemic has caused a lot of patients who do suffer from severe pain from receiving the proper treatment because of all the pill seekers who are abusing the system making it harder for these people to get the care and attention they need.
References
Jones, M.R., Viswanath, O., Peck, J., Kaye, A.D., Gill, J.S., & Simopoulos, T.T. (2018). A Brief History of the Opioid Epidemic and Strategies for Pain Medicine. Pain & Therapy, 7(1), 13-21.
Salani, D., Crenshaw, N.A., Owusu, B., & Gonzalez, J.M. (2018). Pain Management in an Opioid Epidemic: What’s Appropriate, What’s Safe. Clinical Reviews, 28(4), 40-47.
Sharfstein, J.M. (2017). The opioid crisis from research to practice. Milbank Quarterly, 95(1), 24-27.
Tolba, R., Meselhy, E., & Guerra, C.E. (2018). The opioid epidemic and pain medicine specialists: where to begin and what is next? Ochsner Journal, 18(1), 20-22.
Diabetes is a chronic illness that is a result of the pancreas not producing enough insulin or the body is unable to use the insulin in the body effectively. Diabetes can lead to other health complications such as severe hypoglycemia (very low blood sugar) or ketoacidosis (breaking down fat too quickly and making the body acidic), retinopathy (damage to the retinas of the eye), nephropathy (kidney damage), or neuropathy (damage to the nerve system), and cardiovascular disease. According to the World Health Organization, 422 million people have diabetes in the world today. An even more concerning statistic is that 50% of people with diabetes are unaware that they have the disease (Keziah, Gayathri, & Priya, 2019). In order for us to combat this problem, we need to understand what the key components of recognizing this disease are.
What are the signs and symptoms of diabetes?
If you or a loved one are experiencing these symptoms they should see a doctor and be tested right away. These signs or symptoms include:
Frequent Urination
Unexplained Weight Loss
Increased Thirst
Excessive Fatigue
Weight Gain
Slow Healing
Excess Sleep
Blurred Vision
What can I do if I find out I have Diabetes?
If you find out that you do have Type II Diabetes then you will have to make some adjustments in your lifestyle to control or manage the disease. These same lifestyle modifications can be effective in preventing diabetes. The two biggest lifestyle changes that can be made to prevent or combat diabetes are exercise and diet. It is important that you exercise regularly (approximately 120-150 minutes a week) and make modifications to your diet. Dietary changes include eating foods that contain less sugar, increase the amount of fiber intake, and limit carbohydrate intake. Foods to eat include vegetables, fruits, whole grains, proteins, and low-fat dairy products. These simple steps can make a big difference in managing diabetes or preventing the disease altogether.
References
Keziah, V. S., Gayathri, R., & Priya, V. V. (2019). Awareness of the risk factors of diabetes among homemakers – A survey. Drug Invention Today, 11(4), 884–886.
Milne, N., & Di Rosa, F. (2019). The diabetes review: A guide to the basics. Journal of Diabetes Nursing, 23(1), 1–8.
Sanjeevaiah, A., Sushmitha, A., & Srikanth, T. (2019). Prevalence of Diabetes Mellitus and its risk factors. International Archives of Integrated Medicine, 6(3), 319–324.
Kidney Failure: Your Treatment Options
What is Chronic Kidney Disease?
Kidney disease is a serious chronic condition in which the kidneys begin to shut down and not function properly ultimately ending in renal failure. Like other chronic diseases such as heart disease, diabetes, etc., the descent into kidney failure is largely unnoticed in the patient and is not often detected early by medical professionals. Unlike heart disease, there is less funding and public knowledge about kidney health. There are many different causes for kidney disease such as history of diabetes, high blood pressure, genetic predisposition, infection, and many more. Each story is unique to the individual. Kidney disease effects approximately 31 million persons in the US per the American Kidney Fund (2015). Many of those effected with go on to have kidney failure but discussion and research on treatment options should be done early on by the nephrologist and the patient. See below for a video with a great overview on treatment options.
No Action
This is the less discussed and most difficult option to discuss among for medical providers and patients alike because this course of action means that the disease will be allowed to take its course and the end result for the patient will be death. This does not mean that no care will be provided. The patient who chooses this option will continue with their life as it is until they become symptomatic with the disease progression. Once they start to experience the effects of their renal failure, the healthcare team will work with the patient to help provide comfort measures
Transplant
Transplant is the by far the option that most people are aware of and provides that patient with the best results if the transplant is successful. There are two types of transplant options; living donors and deceased donors. Living donors are when a friend, relative, or even stranger donates their kidney for transplantation. The benefits to these transplants are shorter recovery times, planned transplantation, better organ function, and a shorter transplant process (Transplant).
Deceased donors are those who have passed away and decided to donate their organs to those who need them. This is the most common route by which to receive an organ transplantation. The recipient will be placed on a transplant list once approved by a transplant team and the average wait time is 5 to 7 years for a kidney. Many will have to undergo dialysis while waiting for their transplant.
Dialysis is when the patient undergoes chemical and fluid exchanges either through their blood stream of the lining of their abdomen, or peritoneum, which replaces their kidney function by use of an artificial kidney. Dialysis replaces about 15% of the kidneys normal function (DaVita). There are two types of dialysis available
Hemodialysis
Hemodialysis, pictured above, is the process of undergoing exchanges via the blood stream by either a vascular access or central venous catheter. The patient is connected to the machine via blood lines and passes the blood through the artificial kidney cleaning the toxins and excess water from the body over the course of a few hours (Hemodialysis). This is either done in an outpatient dialysis unit three times per week or more frequently at home by the patient and their support system. With the vascular access that is placed by a surgeon, needles are inserted to access the blood. In center dialysis is the preferred method of dialysis in the United States. At home provides the most flexibility for the patient as far as scheduling and being able to do it in the comfort of one’s own home. Hemodialysis also requires the patient to adhere to a strict renal diet often in combination with other diets like heart or diabetic depending on the patients co morbidities.
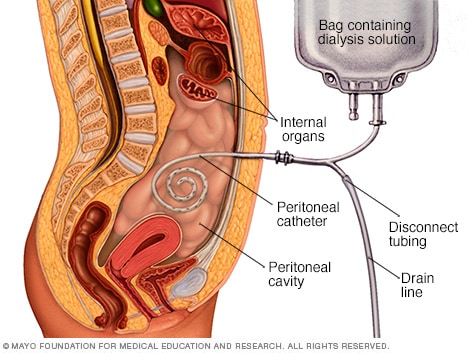
Peritoneal Dialysis Peritoneal dialysis is a mode of dialysis that is done at home by the patient and their support system typically overnight. A catheter is inserted into the lining of the abdomen called the peritoneum, and that catheter is used for the exchange of the dialysate fluid that conducts the dialysis process. When done overnight, there are as many as four or more exchanges being made after hooking up to the catheter. Peritoneal dialysis provides the greatest freedom for the patient as it is done while they are sleeping, has the least restricted diet, and is also the gentlest on the body as is slowly exchanges the fluid and toxins over a longer period of time and blood is not drawn from the body to conduct the dialysis.
There are many different options of how to treat your Renal Failure. Deciding which mode of treatment is right for you is purely personal as only you know what fits best in your life. Be sure to have an open discussion with your nephrologist about all treatment options to decide which fits your lifestyle the best.
Dialysis linked to dementia in seniors [Digital image]. (2018, September 4). Retrieved May 8, 2019, from https://www.health24.com/Medical/Dementia/News/dialysis-linked-to-dementia-in-seniors-20180815
Hemodialysis. (2018, January 01). Retrieved May 8, 2019, from https://www.niddk.nih.gov/health-information/kidney-disease/kidney-failure/hemodialysis
Peritoneal dialysis [Digital image]. (n.d.). Retrieved May 8, 2019, from https://www.davita.com/treatment-services/dialysis/what-dialysis-can-and-cannot-do
Transplant. (n.d.). Retrieved May 8, 2019, from https://www.barnesjewish.org/Medical-Services/Transplant/Kidney-Transplant/Kidney-Transplant-Options
What dialysis can and cannot do. (n.d.). Retrieved May 8, 2019, from https://www.davita.com/treatment-services/dialysis/what-dialysis-can-and-cannot-do
Deep Vein Thrombosis (DVT) happens when blood turns into a clot in a vein in the body. These clots can block off the whole vein or just a piece of the vein in the body. Clots can happen anywhere in the body but most commonly happen in the calf. When staying at the hospital, no matter how long of a stay, a DVT can happen and to anyone. Keeping informed about ways to prevent these clots can decrease your hospital visit. Below is a helpful video on DVT prevention from Brigham Health which is breaks down the information above.
DVT Prevention
A few ways to prevent blood clots includes walking frequently, compression stockings, intermittent pneumatic compression devices, and low molecular weight heparin. Some of these ways may be new terms. Compression stockings and intermittent pneumatic compression devices are ways to decrease swelling in the patients legs and improve blood flow in the legs. The video below on DVT pumps: otherwise known as intermittent pneumatic compression devices are seen in the hospital setting and is a great tool to help prevent blood clots. This video is a great tool to learn about these devices.
Low molecular weight heparin may be a new term too. This medication has other names too, such as Lovenox or enoxaparin. The medication comes as an injection (shot) that helps thin the blood. Below is an informational video regarding heparin shots needed to help prevent blood clots. This video is very instructional and easy to understand, however, the video suggests to recap after injecting the medication. This is a big no no and can cause patients to accidentally restick themselves with the needle. Also, using alcohol swabs is correct, the video forgets to mention to wipe the area for fifteen seconds and dry for fifteen seconds before giving the injection. Although this video seems like a great resource for at home injections, it is always best to learn information and techniques from your doctor.
Resources you can trust
Below are some educational resources that are easy to read and helpful places to go to learn about preventing blood clots.
Kaur, M., Yadav, K., Yadav, V., Gupta, B., & Misra, M. (2012). Deep vein thrombosis (DVT) prophylaxis: awareness or ignorance amongst staff personnel. International Journal of Nursing Education, 4(1), 32–34.
O’Brien, A., Redley, B., Wood, B., Botti, M., & Hutchinson, A. F. (2018). STOPDVTs: Development and testing of a clinical assessment tool to guide nursing assessment of postoperative patients for Deep Vein Thrombosis. Journal of Clinical Nursing (John Wiley & Sons, Inc.), 27(9–10), 1803–1811.
Van Wicklin, S. A. (2011). Implementing AORN Recommended Practices for Prevention of Deep Vein Thrombosis. AORN Journal, 94(5), 443–456.