
History
Since ancient times, humans have used the leaves and flowers from the cannabis plant as herbal medicine, manufacturing of textiles and during religious/spiritual ceremonies. During the 1800s a physician by the name of Sir William Brooke O’Shaughnessy set off to India and researched the medicinal properties of Opium and Cannabis. O’Shaughnessy is noted to have discovered therapeutic purposes with the use of Cannabis and is also noted for co-finding intravenous fluid and electrolyte replacement therapy for Cholera patients. During his many Cannabis studies, he successfully treated a 40-day old infant who suffered from febrile seizures (convulsions caused by fever) with Cannabis. Much of his research focused on anesthesia and pain relief.
Following these discoveries from the time of about 1850-1937 over the counter (OTC) tinctures of Cannabis where sold in pharmacies to treat everything from gout to hysteria. If you suffered from an ailment during these time you were most likely treated with some sort of concoction made from Cannabis and other pharmacological remedies.
On August 2, 1937, President Franklin D. Roosevelt enacted the Marihuana Tax Act of 1937 in the United States of America. This legislative bill didn’t exactly prohibit the use of marijuana. The bill simply made every person who imports, manufactures, compounds, produces, sells, deals in, dispenses, prescribes, or gives away marijuana to pay a hefty tax. The imposed tax was so high that physicians, pharmacists, and other healthcare professionals could not afford to pay, thus resulting in an attack on patient rights and healthcare as a whole. The Marihuana Tax Act of 1937 was overturned by the Supreme Court on May 19, 1969, due to its violation of the Fifth Amendment.
Not soon after overturning the Marihuana Act of 1937 the Controlled Substance Act of 1970 was signed into law by President Richard Nixon on October 27, 1970. This statute makes it illegal to manufacture, import, possess, use and distribute substances which are placed into five classifications. Classification is based on three factors: potential for abuse, accepted medical use, and safety/potential for addiction. According to the Drug Enforcement Administration (DEA), and the Food and Drug Administration (FDA) marijuana is classified as a Schedule I controlled substance. These two organizations determine what is added or removed. Some other drugs also considered a Schedule I drug include:
- Alpha-methyltryptamine (aMT)
- Benzylpiperazine (BZP)
- Cathinone
- Dimethyltryptamine
- Etorphine
- Gamma-hydroxybutyrate (GHB)
- Heroin
- Ibogaine
- Lysergic acid diethylamide (LSD)
- Methylenedioxymethamphetamine (MDMA)
- Mescaline
- Methaqualone
- Peyote
- Psilocybin or psilocin
- This is not a complete list of Schedule I drugs and is a very brief history.
To put a perspective on things Crack Cocaine is classified as a Schedule II substance, implying it is safer to use than marijuana. In fact, most drugs linked to the opioid epidemic our nation is facing are classified as a Schedule II drug. It appears the FDA and DEA are not applying their three factors of classification regarding drugs accordingly. Maybe O’Shaughnessy was on to something? Maybe Cannabis can be used for pain relief. Or maybe Cannabis should be reclassified?
What is Medical Cannabis?
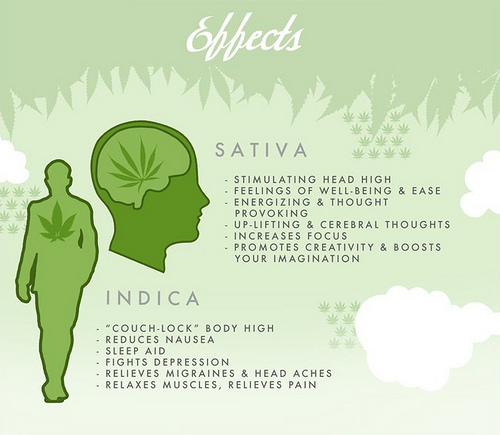
The term cannabis and marijuana are often used interchangeably. Cannabis is a flowering plant that includes numerous subspecies. The most common subspecies are Cannabis Sativa and Cannabis Indica. Cannabis is considered a psychoactive drug which is thought to affect one’s mind or behavior. The main psychoactive ingredient in Cannabis is delta-9 tetrahydrocannabinol, commonly known as THC. Within our bodies scientists have discovered something called the endocannabinoid system. This system is essentially a chemical messegenr within our bodies that react with the cannabinoid receptors CB1 and CB2 and have physical and psychological effects on the body. But I am not here to get into scientific details.
“Research”
Most research I come across clearly states more research is needed in the field of medical marijuana for safety, efficacy, etc. However certain factors make it extremely limited. Currently, in the United States, only one facility is federally licensed by the DEA to cultivate and research marijuana. Although 25 applications have been pending since 2017 based on a 2016 statement by the DEA supposedly granting more access. Naturally, it’s all a very corrupt system. While marijuana is federally illegal, the government has no problem supplying federal money or “research” marijuana as long as your agenda lines up with theirs. Meaning that most research doesn’t go into seeing if it can help ease pain or other diseases. It goes towards research geared at what it has been doing for the last 80 or so years. Trying to instill fear into the American people.

By: Julie Mac
The War On Drugs
Let’s face it. The United States is losing the War on Drugs. Is the government to blame? Pharmaceutical Companies? Consumers? Opioid-related deaths are the number one preventable death in the United States currently. Even the medicine used to treat opioid addiction can lead to overdose and death. In one 21-month study that took place in the state of Arizona which included habitual and non-habitual opioid users. The study shows that opioid users reduced their consumption from 83.8% to 44.8% or stopped filling their prescriptions at all while using medically prescribed cannabis for pain relief. Patients also found significant relief from their pain symptoms and none reported any serious side effects. The most intriguing study to me is that 64% of medical cannabis (MC) users decreased their opioid drug use and where able to manage their pain more effectively. Another study showed that the use in MC patients reduced the number of opioid overdoses, therefore increasing mortality rates within those populations. Ingestion methods in this study included smoking of the cannabis flower, edibles, vaporization, and topical oils. I like how this study has things you can read that the participants had to say. Some like the fact that MC is not destroying their liver like opioids can and others talk about how they went from taking 180 Vicodin a month which made them sick to their stomach and now they rely on MC because the effects last longer on their pain with fewer side effects from opioids.
Conclusion
The current lack of research is severely hindering the potentials that MC could have on pain research and other alternative therapies. A great start would be getting the government to declassify Cannabis from a Schedule I to a Schedule II to allow for more research. Then we can focus on medical research and benefits and ultimately curb the opioid epidemic the nation is having due to drugs that were not intended for everyday consumption by the general population.
References
Bruce, D., Brady, J. P., Foster, E., & Shattell, M. (2018). Preferences for Medical Marijuana over Prescription Medications Among Persons Living with Chronic Conditions: Alternative, Complementary, and Tapering Uses. Journal of Alternative & Complementary Medicine, 24(2), 146–153.
Medical cannabis effective in treating a wide range of health conditions: Researchers have found that medical cannabis provides immediate symptom relief across dozens of health symptoms – with minimal negative side-effects. (2018). Canadian Nursing Home, 29(4), 13–14.
Vigil, J. M., Stith, S. S., Adams, I. M., & Reeve, A. P. (2017). Associations between medical cannabis and prescription opioid use in chronic pain patients: A preliminary cohort study. PLoS ONE, 12(11), 1–13.